Luteal Phase Defects and Fertility: A Guide to Understanding Your Cycle Window

What if the reason you aren't seeing a positive pregnancy test has nothing to do with your ovulation day and everything to do with what happens ten days later? For many women, the struggle to conceive isn't about the egg's release, but rather the waiting room period that follows. Research shows that nearly 9% of ovulatory cycles in regularly menstruating women involve a short luteal phase, which can complicate the link between luteal phase defects and fertility. If you've felt dismissed by doctors because your cycle is borderline or you're anxious about mid-cycle spotting, you're not alone in your frustration.
You deserve a clear answer to whether your cycle length is standing in the way of a healthy pregnancy. It's understandable to feel overwhelmed when your body seems to be rushing through its most important phase. This guide will help you understand the critical 10-day threshold and provide evidence-based steps to optimize your progesterone levels for a successful pregnancy. We'll explore actionable ways to confirm ovulation, along with the specific supplements and lifestyle changes that support a robust uterine environment. By the end, you'll have a clear roadmap to help your body sustain a pregnancy.
Key Takeaways
- Learn why a phase length of 10 days or fewer is the clinical marker for a defect and how it impacts your "window of receptivity."
- Understand the relationship between luteal phase defects and fertility, specifically how progesterone transforms the uterine lining for successful embryo implantation.
- Discover how to use Basal Body Temperature (BBT) tracking to confirm your thermal shift and identify subtle signs like pre-menstrual spotting.
- Explore evidence-based support strategies, from medical progesterone supplements to nutritional co-factors like Vitamin B6 and Zinc that promote cycle health.
- Gain clarity on when to transition from home tracking to consulting a reproductive specialist with your charted data.
What is a Luteal Phase Defect? Defining the Conception Window
Most fertility conversations focus heavily on the lead-up to ovulation, but what happens after the egg is released is just as vital for a successful pregnancy. What is the Luteal Phase? It's the specific timeframe beginning the day after ovulation and ending the day before your next period. While the first half of your cycle can vary significantly due to stress or lifestyle changes, your luteal phase is usually quite stable. If this window is consistently too short, it creates a significant hurdle for luteal phase defects and fertility.
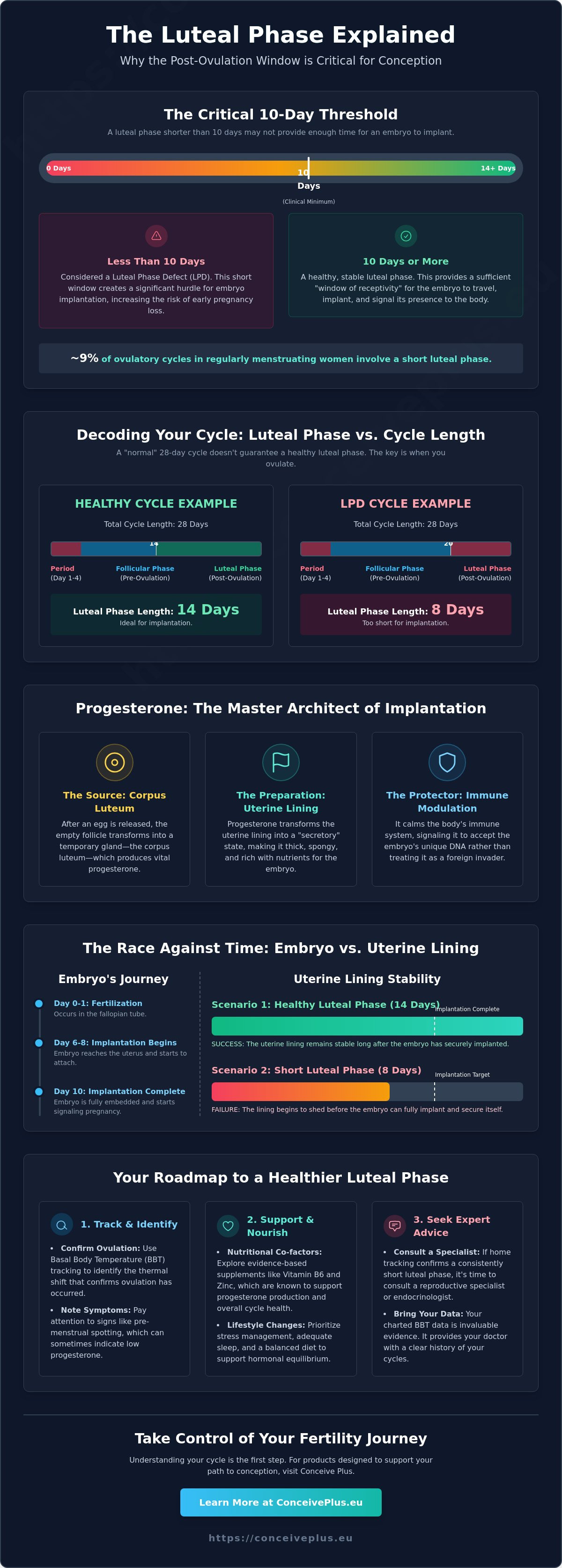
Clinical standards generally define a luteal phase of 10 days or less as a "defect" or deficiency. This 10-day threshold is critical because an embryo typically takes 6 to 10 days to travel down the fallopian tube and find a spot to implant in the uterine wall. If your hormonal "support system" collapses before the embryo can settle in, the uterine lining begins to shed, and a pregnancy cannot be sustained. Even if fertilization occurs, a short window often results in what looks like a typical period, leaving many women unaware that a conception attempt was even in progress.
To better understand how this cycle window functions and why its length matters, watch this helpful video:
The Physiology of the Corpus Luteum
The magic of the second half of your cycle happens because of the corpus luteum. Once a follicle releases its egg, that empty shell doesn't just disappear; it transforms into a temporary gland called the corpus luteum. This "yellow body" is a hormone factory responsible for pumping out progesterone in rhythmic pulses. Under the control of Luteinizing Hormone (LH), progesterone prepares the womb for a guest. For a pregnancy to stick, this gland must stay active and healthy for at least 10 days to ensure the uterine environment remains stable and nutrient-rich.
Luteal Phase Deficiency vs. A Short Cycle
It's a common mistake to assume a short cycle always means a luteal phase defect. You might have a 24-day cycle that is perfectly healthy if you ovulate on day 12. However, if you have a "standard" 28-day cycle but don't ovulate until day 20, you only have an 8-day luteal phase. This is the core issue with luteal phase defects and fertility. The problem usually stems from one of three areas: the follicle didn't develop well enough before ovulation, the corpus luteum isn't producing enough progesterone, or the uterine lining isn't responding to the hormones it receives. Because of these variables, having a regular period doesn't always guarantee your luteal phase is long enough to support a growing embryo.
How Luteal Phase Defects Impact Fertility and Implantation
Once you understand the 10-day threshold, the next question is why that specific timing matters so much. Successful conception relies on a synchronized dance between the developing embryo and the uterine lining. This period of peak readiness is known as the "window of receptivity." If the timing is off even by a few days, the embryo arrives to find a closed door, making the connection between luteal phase defects and fertility a critical factor for anyone trying to conceive.
Progesterone is the architect of this window. During the first half of your cycle, estrogen builds a "proliferative" lining, essentially thickening the walls of the uterus. After ovulation, progesterone takes over to transform that lining into a "secretory" state. This change fills the lining with glycogen and specialized proteins that act as the embryo's first meal. Just as importantly, progesterone acts as an immune-modulator. It signals your body's immune system to accept the embryo's unique DNA rather than treating it like a foreign invader. Without this shift, the environment remains hostile to implantation.
The Implantation Timeline
After fertilization in the fallopian tube, the embryo begins a journey that lasts about five to six days. It only attempts to anchor once it reaches the blastocyst stage. Implantation typically occurs between days 6 and 10 post-ovulation, right in the heart of the luteal phase. If your phase ends at day 8 or 9, the lining begins to break down before the embryo can even send the hormonal signal (hCG) to stop your period. It's a literal race against the clock. When the cycle is too short, you might experience early pregnancy loss that feels like a heavy or slightly late period, further complicating the link between luteal phase defects and fertility.
Endometrial Resistance: When Hormones Aren’t Enough
Sometimes, blood tests show "normal" progesterone, yet a woman still struggles with a short cycle. This is often due to progesterone receptors in the lining not responding correctly. The American Society for Reproductive Medicine discusses these complexities in their committee opinion on Diagnosing and Treating Luteal Phase Deficiency. If the receptors are blocked or sluggish, the lining doesn't "hear" the signal to stay put. A thin or poorly developed lining fails to provide the structural support and blood supply necessary for a blastocyst to anchor and thrive. Supporting your body with targeted fertility support can help create a more receptive environment for these delicate early days.
Identifying Symptoms and Tracking Your Luteal Phase at Home
Recognizing the signs of a hormonal imbalance requires more than just marking the start of your period on a calendar. While many doctors focus on the total cycle length, your data tells a much more nuanced story about the "wait" period. To build a clear picture of luteal phase defects and fertility, you need to track at least three consecutive cycles. This consistency helps you distinguish between a one-off stressful month and a persistent pattern that might be interfering with your ability to conceive.
The first step is pinpointing the exact day of ovulation. You can use an ovulation calculator to estimate your fertile window, but confirming the event is essential. By combining Luteinizing Hormone (LH) surge data from testing strips with daily temperature monitoring, you can identify exactly when your luteal phase begins. This data is your best defense against being unheard by medical professionals, as it provides concrete evidence of your body's timing.
Symptoms You Shouldn’t Ignore
Your body often sends subtle signals when progesterone levels are insufficient. One of the most common red flags is brown or pink spotting that occurs three to five days before your actual period begins. This isn't just "early menstruation." It's a sign that the corpus luteum is failing early, causing the uterine lining to destabilize. Other signs include:
- Cycle Length Fluctuations: Total cycles shorter than 25 days or those that vary wildly in length each month.
- Hormonal Mood Shifts: Significant drops in mood or libido immediately after ovulation, which can signal a sharp progesterone crash.
- Physical Markers: A lack of breast tenderness or a sudden drop in basal temperature just a few days after it rose.
Practical Tracking Tools
Basal Body Temperature (BBT) is one of the most reliable ways to verify the health of your luteal phase. After ovulation, your temperature should rise and stay elevated because progesterone is thermogenic. You can use the "Coverline" method to visualize this shift; your temperature should remain above this line for at least 11 days. If you see a "thermal shift" that lasts only 8 or 9 days, it's a strong indicator of a defect. For even more precision, consider using Progesterone (PdG) test strips. Unlike a single blood test, these urine-based strips can confirm that progesterone remained high enough for several days following ovulation, ensuring the window of receptivity stayed open long enough for an embryo to anchor. Understanding these patterns is the first step in addressing luteal phase defects and fertility concerns effectively.
Solutions and Support Strategies for Luteal Phase Health
Improving your cycle window isn't just about adding more hormones. It's about creating an environment where your body can sustain its own natural production. While the diagnosis of luteal phase defects and fertility challenges can feel daunting, many women see improvements by focusing on the foundation of their cycle. A healthy luteal phase actually begins during the follicular phase. If the follicle doesn't develop robustly before ovulation, the resulting corpus luteum won't have the strength to produce enough progesterone. Supporting egg quality from day one is often the most effective way to ensure a longer, stronger second half of your cycle.
Lifestyle adjustments play a surprising role in hormone stability. When you're under chronic stress, your body prioritizes the production of cortisol. Because progesterone and cortisol share the same molecular precursor, pregnenolone, your body may "steal" resources to manage stress, leaving very little for your uterine lining. Reducing high-intensity stressors and prioritizing sleep can help protect your progesterone levels from this metabolic diversion. Consistency is key here. It often takes two to three cycles of dedicated support to see a measurable shift in your BBT charts.
Nutritional and Supplemental Support
Specific nutrients act as co-factors that help the corpus luteum function at its peak. Vitamin B6 is particularly well-documented for its ability to regulate hormonal activity and lengthen the luteal phase. Meanwhile, antioxidants like Vitamin C and Vitamin E protect the corpus luteum from oxidative stress, ensuring it doesn't break down prematurely. Zinc is another essential mineral that supports the pituitary gland in releasing the hormones that trigger ovulation in the first place. For those looking for a streamlined approach, fertility support bundles offer a way to ensure you're getting these critical nutrients in the correct ratios for cycle health.
Medical Treatments vs. Natural Support
If lifestyle and nutritional changes aren't enough, medical interventions can bridge the gap. Your doctor might suggest a "Day 21" progesterone blood test, though it's more accurate to call it a "7 days post-ovulation" test. If levels are low, vaginal progesterone suppositories are often preferred over oral versions because they deliver the hormone directly to the uterine lining with fewer systemic side effects. In some cases, an hCG trigger shot is used during ovulation to "boost" the corpus luteum's performance later in the month. Balancing these clinical tools with natural fertility support provides a comprehensive strategy to reclaim your conception window.
Navigating Your Fertility Journey: Next Steps and Expert Advice
You've spent months tracking temperatures and counting days. It's exhausting. While the link between luteal phase defects and fertility is clear, the emotional toll of "cycle-watching" is often overlooked. If you've tracked for three cycles and consistently see a phase under 10 days, it's time to transition from home monitoring to professional consultation. You don't have to do this alone. With 1 in 6 adults worldwide affected by infertility according to current global statistics, specialists are well-versed in these common hormonal hurdles.
The psychological impact of tracking every minor symptom can lead to significant anxiety. It's easy to feel like your body is failing you when the "thermal shift" doesn't last as long as you'd like. Remember that your data is a tool for empowerment, not a reason for self-criticism. Taking a break from digital apps for a few days or focusing on non-fertility goals can help manage the cortisol levels that we've already seen can negatively impact your progesterone production. LPD is often one of the most treatable fertility hurdles once you have the right team behind you.
Talking to Your Healthcare Provider
When you walk into a reproductive endocrinologist's office, your data is your best advocate. Bring your BBT charts and LH surge records to show exactly when your "window" is closing. Many doctors might dismiss a cycle that's "borderline" at 11 days, but if you're experiencing mid-cycle spotting, your concerns are valid. Ask specific questions: "Is my progesterone peaking at the right time?" or "Does my lining show secretory changes?" The goal of treatment is extending the window for life to take hold.
Finding the Right Support System
You're more than just a collection of hormonal data points. A holistic approach that combines clinical science with proper nutrition and emotional support often yields the best results. Don't underestimate the power of community. Connecting with others who understand the frustration of a short cycle can significantly lower your stress levels. You can also look for special offers on high-quality tracking tools and supplements to ease the financial burden of your journey. Combining these resources ensures you're supporting your body from every possible angle.
Final encouragement: luteal phase issues are frequently resolved with straightforward interventions. Whether the fix is a targeted supplement or a prescribed progesterone support, these adjustments can make a world of difference. Your proactive tracking has already put you steps ahead in the process. Take a deep breath. You've done the hard work of understanding your body's unique rhythm, and now you have the knowledge to move forward with confidence.
Empowering Your Path to Conception
You now have the knowledge to determine if a short cycle is impacting your journey. By monitoring your thermal shift and recognizing early spotting as a potential sign of low progesterone, you can advocate for your reproductive health more effectively. Successfully managing luteal phase defects and fertility isn't just about counting days on a calendar. It's about optimizing your body's internal environment to ensure every cycle has the best possible chance for life to take hold.
Taking the next step toward a healthy pregnancy often starts with the right nutritional foundation. Our comprehensive range is developed by Harvard doctors and specifically formulated to support the natural conception process. Used by millions of couples in over 70 countries, these tools are designed to help you bridge the gap between ovulation and a positive test. You've already done the hard work of learning your rhythm; now it's time to give your body the support it deserves.
Shop All Fertility Support Products to begin your next cycle with confidence. Your commitment to understanding your body is a powerful part of your story, and every step forward brings you closer to your goal.
Frequently Asked Questions
Can I get pregnant with a 9-day luteal phase?
It's possible to conceive with a 9-day luteal phase, but the odds are significantly lower because the embryo has less time to implant. Since implantation typically occurs 6 to 10 days after ovulation, a 9-day window often causes the uterine lining to shed before the embryo can successfully anchor. This creates a challenging environment for luteal phase defects and fertility, often requiring support to extend the cycle.
Does stress cause a luteal phase defect?
Chronic stress is a well-documented cause of shortened luteal phases because it disrupts the delicate hormonal balance required for ovulation. When your body is under pressure, it prioritizes cortisol production, which can suppress the surge of Luteinizing Hormone (LH) needed to form a strong corpus luteum. Reducing stress through lifestyle changes can sometimes help restore a normal cycle length and improve your chances of conception.
How can I naturally increase my progesterone during the luteal phase?
You can support progesterone production by prioritizing nutrients that fuel the corpus luteum, such as Vitamin C, Zinc, and Magnesium. Eating enough healthy fats and ensuring you don't over-exercise can also prevent the hormonal crashes that lead to a short cycle. These natural adjustments help maintain the "secretory" lining needed for an embryo to thrive during the second half of your month.
Is spotting a week before my period a sign of a luteal phase defect?
Early spotting is a classic clinical red flag that your progesterone levels are dropping prematurely. This brown or pink discharge indicates that the uterine lining is starting to break down too soon, which can prevent an embryo from implanting. If you notice spotting 5 to 7 days before your period, it's a strong indicator that you should track your cycle more closely for signs of deficiency.
What is the best time to test progesterone levels?
The ideal time for a blood test is exactly seven days after you ovulate, which is when progesterone should be at its peak. While many clinics call this a "Day 21" test, it's only accurate on that day if you ovulated on Day 14. If you ovulate later, testing on Day 21 will show artificially low levels that don't reflect your actual hormonal health.
Can Vitamin B6 really lengthen my luteal phase?
Vitamin B6 is widely recognized for its role in regulating hormonal activity and has been shown to help extend the luteal phase for some women. It works by improving the quality of the follicle before it's released, which leads to a more robust corpus luteum. Many women find that consistent B6 supplementation over three months can add one or two vital days to their cycle window.
What happens if my luteal phase is too long?
A luteal phase that exceeds 17 days is usually the first sign of pregnancy, as the body continues producing progesterone to support the embryo. If a pregnancy test is negative, a very long phase could indicate a corpus luteum cyst or a hormonal imbalance that prevents the lining from shedding. While less common than short phases, a consistently long window should be discussed with a reproductive specialist.
Is a luteal phase defect the same as early menopause?
No, these are two very different reproductive health issues. A luteal phase defect is a treatable hormonal imbalance regarding how your body sustains a cycle, while early menopause is the loss of egg function. Understanding the difference is vital for managing luteal phase defects and fertility, especially since 1 in 6 adults globally face infertility challenges that require specific, targeted diagnoses rather than general assumptions.














